Chronic Disease Management Programmes in Polyclinics
Multi-disciplinary team
The framework in the development of the disease management programme included identifying the diseases and defining the target population, organising a multi-disciplinary team led by a clinician champion, defining the core components, treatment protocols and evaluation methods, defining the goals, and measuring and managing the outcomes. Primary healthcare centres, or polyclinics, are run by teams of family physicians, medical officers, nurses, case managers, health educators, dieticians, pharmacists, clinical administrators and medical social workers. The establishment of the clusters has provided a setting in which structured disease management could be readily implemented.
All the current 18 government polyclinics have structured disease management programmes that are team-based and led by family physicians (known as clinician champions). The functional integration of these healthcare elements within each cluster under a common administrative and professional management, and the development of common clinical information systems greatly facilitate the implementation of the disease management programmes.
Multi-disciplinary decision support protocols have been developed in conjunction with hospital specialists to provide consistent integrated pathways and to facilitate the referral systems. Case managers have been recruited and trained in developing clinical pathways and performing discharge planning for inpatients and utilisation review for outpatient care in the hospitals.
Clinical case managers in primary care, recently introduced into polyclinics, work closely with patients on the lifestyle and medication changes required to achieve targets, which is a prominent feature of most successful chronic disease programs. The case manager is usually a nurse or nurse practitioner with additional training or experience in a particular chronic disease care and in techniques to help patients become more capable self-managers of their illness. The nurses personally “manage” patients by protocol, adding clinical and self-management skills as well as greater intensity of care.
Chronic disease management
There are currently two established disease management programmes in the polyclinics, i.e. Enhanced Primary Care Asthma Clinic and Family Physician Clinic (also known as Diabetes, Hypertension and Lipid or DHL Clinic). In the polyclinics, infrastructures built for the chronic disease management programmes would include well-equipped consultation rooms for individual (one-to-one) health counselling/education, smoking cessation counselling, fundus camera for diabetic retinal photography, diet counselling, and feet check; each man by a trained nurse.
Spacious air-conditioned waiting areas with educational video presentations and printed materials readily available for patients to consume. Not all patients with chronic diseases are seen in these clinics. Patients are stratified and those with sub-optimal control who fulfil criteria in their decision support tool are given appointments to follow-up in these chronic care clinics, for example, asthmatic patients on regular high-dose steroid inhalers or recently admitted for acute exacerbation, diabetic patients with HbA1c of 8% or more, and complicated patients with two or more chronic conditions.
Once their conditions are stabilised, patients have an option to be referred back to their previous primary care doctors.
Clinical information system
The healthcare team in these programmes is continuously trained and supported with practical decision protocols, which are constantly updated by the team. Feedback and comments from the team members are always taken into consideration. The team conducts monthly plan-do-study-act (PDSA) cycles looking at clinical outcome (disease control) indicators, such as reductions in HbA1c, blood pressure, microalbuminuria, as well as improvement in care processes, such as performance of retinal or feet examinations in diabetics and peak expiratory flow rate in asthmatics.
This is possible because all patients with chronic disease have their socio-demographic data documented in the highly secured web-based information system that is linked to the clinical information system and accessible to all polyclinics and hospitals from the same cluster. The all-in-one information system registers the patient flow from the appointment system to consultation rooms (the queue management system and scheduled examinations), laboratory (reminder system and clinical laboratory indicators), radiology, pharmacy and consolidated payment at the end of each clinic visit.
Self-management Tool
Patients with one or more chronic diseases are encouraged to purchase a self-management booklet (S$5 each). A trained nurse clinician demonstrates the usefulness of the booklet via video presentation and counselling and teaches the patient individually how to use it at home for self-monitoring and management. All asthmatic patients are taught to use the practical and patient-friendly asthma action plans and diaries.
Clinical vs Organisational Management Skills
There is another new paradigm shift in polyclinic management in conjunction with chronic disease management. In the past family physicians were primarily focusing on polishing clinical skills and updating clinical management. From what a family physician can do for his circle of patients, they are now trained to bring better care to masses of people through improved management skills. Directors of polyclinics who are usually senior consultant family physicians are now regularly attending management and leadership courses.
Support from the Ministry of Health
The Ministry of Health Singapore establishes National Disease Registries in coronary heart disease, cancer, stroke, myopia and kidney failure, which become valuable sources of clinical and outcomes data. In partnership with expert groups, national committees and professional agencies, the Ministry produces clinical practice guidelines that assist doctors and healthcare professionals in managing important aspects of key diseases better. Most importantly, the Ministry has committed funds to support selected National Disease Management programmes and allows qualified patients to utilise their national health insurance scheme, Medisave to help pay for these disease management programmes, up to a maximum of S$300 annually.
The Ministry monitors and publishes regularly the performance, cost and effectiveness of these disease management programmes so that patients can make informed choices when selecting their health providers. This steers patients and doctors towards the strategy of preventive maintenance to stop or slow down the deterioration of chronic medical conditions. All registered government family physicians and private general practitioners who have an interest in chronic care are encouraged to participate in these disease management programmes.
The list of doctors’ names and their effectiveness are published on the ministry’s website. Patients with any of these chronic diseases are advised to register with these doctors, who will presumably be their Family Physicians. The cost and health outcomes of these patients are monitored and important data is published at the website for both patients and doctors to learn from one another.
In conclusion, Singapore’s health care has taken a major leap and invested a large amount of money and workforce in chronic disease management. These changes attempt to integrate population perspectives and person-centred perspectives. Primary health care teams can play a lead role in chronic illness care, but healthcare organisation system support and policy are critical to its success.
Vanda Clinic Management System
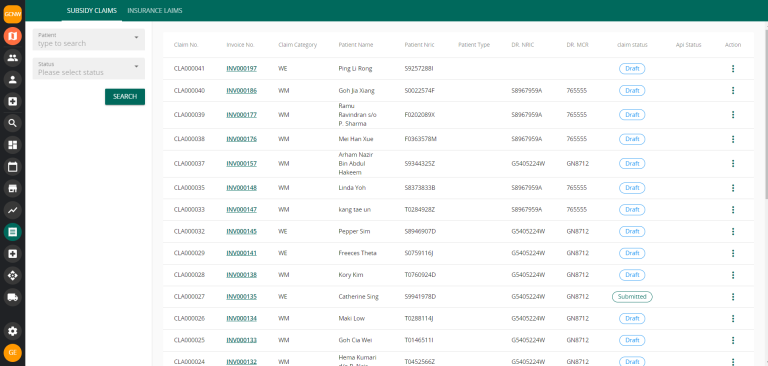
Using Vanda, you are able to save patient’s chronic diseases and past medical history to refer back to anytime